Central Retinal Vein Occlusion
Central retinal vein occlusion, also known as CRVO, is a condition in which the main vein that drains blood from the retina closes off partially or completely. This can cause blurred vision and other problems with the eye.
Causes and Risk Factors: Most patients with CRVO develop it in one eye. And, although diabetes and high blood pressure are risk factors for CRVO, its specific cause is still unknown. What we do know is that CRVO develops from a blood clot or reduced blood flow in the central retinal vein that drains the retina. And we have learned that a large number of conditions may increase the risk of blood clots. Some eye doctors advise testing for them.
However, it is not certain how these health conditions are related to CRVO—and some of them, if diagnosed, have no agreed-to or necessary recommended treatment.
Many eye doctors do not advise testing for a CRVO in one eye, but do recommend a visit with a family doctor to be sure there is no diabetes or high blood pressure.
CRVO that occurs in both eyes at the same time can be related to systemic disease; in these cases, a tendency toward abnormal blood clotting is definitely more common and medical testing to detect so-called “hypercoagulable states” is indicated. While some eye doctors coordinate such testing, most refer patients to their family doctors, internists, or hematologists (physicians specializing in diseases of the blood) for testing.
WHAT IS THE RETINA?
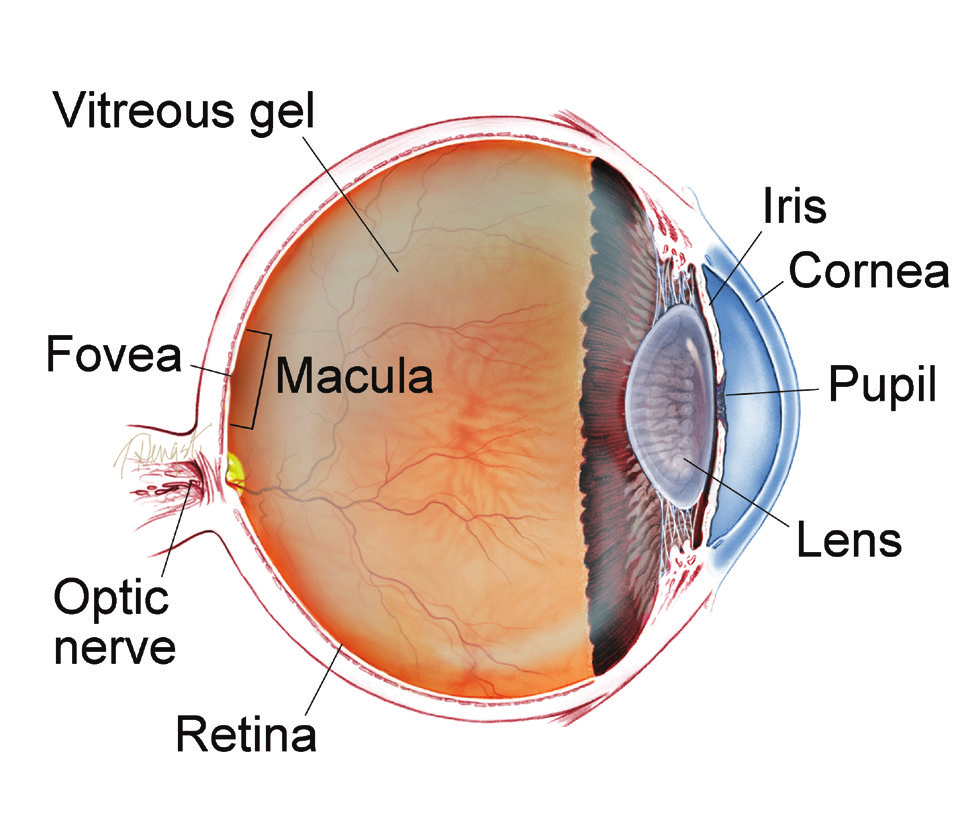
THE RETINA is a thin layer of light-sensitive nerve tissue that lines the back of the eye (or vitreous) cavity. When light enters the eye, it passes through the iris to the retina where images are focused and converted to electrical impulses that are carried by the optic nerve to the brain resulting in sight.
Diagnostic Testing: CRVO (Central Retinal Vein Occlusion
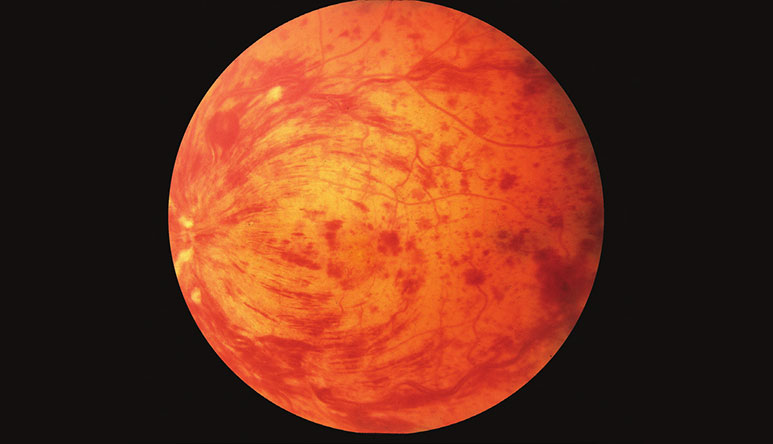
) is typically a clinical diagnosis—that is, one based on medical signs and patient-reported symptoms. When a retina specialist looks into the eye, there is a characteristic pattern of retinal hemorrhages (bleeding) and a diagnosis is made (Figure 1).
Common conditions that can take on an appearance of CRVO include diabetic retinopathy (retina disease) and retinopathy related to low blood counts, such as anemia and thrombocytopenia (a deficiency of blood platelets).
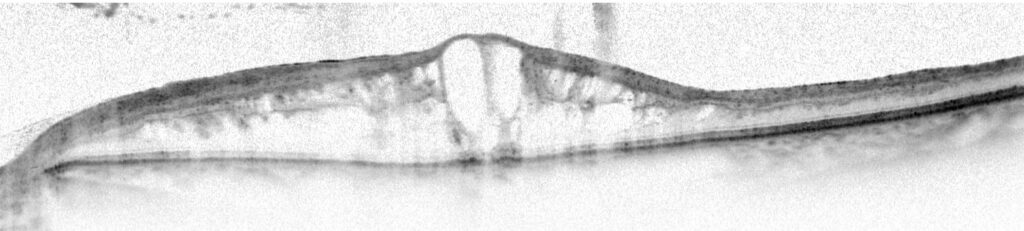
Swelling of the center of the retina, called macular edema is common, and to detect this and measure the amount of swelling, an optical coherence tomography (OCT) image is often obtained (Figure 2). To help distinguish CRVO from conditions that may mimic it, and
Figure 1
CRVO with Flame Hemorrhages Jeffrey G. Gross, MD. Retina Image Bank 2012; Image 968. ©American Society of Retina Specialists.

Figure 2
OCT of an acute CRVO with severe macular edema. Image courtesy of John Thompson, MD to assess closure of small blood vessels, or to search for or confirm growth of new abnormal vessels, fluorescein angiography (FA) imaging may be performed.
Prognosis and Treatment: CRVO has a better prognosis in young people. In older patients who receive no treatment, about one-third improve on their own, about one-third wax and wane and stay about the same, and about one-third get worse. If there is macular edema, it may improve on its own.
In patients with CRVO, vascular endothelial growth factor (VEGF) is elevated; this leads to swelling as well as new vessels that are prone to bleeding. The most common treatment, based on results from powerful randomized clinical trials, involves periodic injections into the eye of an anti-VEGF drug to reduce the new blood vessel growth and swelling. Anti-VEGF drugs include bevacizumab (Avastin®), ranibizumab (Lucentis®), and aflibercept (Eylea®).
Although anti-VEGF drugs reduce the swelling, they are not a cure. As the drug leaves the eye and moves into the bloodstream, the effect in the eye wears off, so re-injection is often needed. A rare lucky patient needs only one injection, but the norm is a series of periodic injections over the course of a few years.
Another option for treating macular edema from CRVO is with an injection of intraocular steroid. This could be either a liquid steroid called triamcinolone or a small steroid pellet called dexamathasone implant (Ozurdex(R)). The steroid injections typically last several months, but can cause elevated intraocular pressure requiring eye drops or increased rate of cataract formation.
Ischemic (pronounced is KEY mick) and Non-ischemic CRVO:
CRVO comes in 2 types:
- Non-ischemic CRVO—a milder type characterized by leaky retinal vessels with macular edema
- Ischemic CRVO—a more severe type with closed-off small retinal blood vessels
Patients with ischemic CRVO have worse vision with less chance for improvement. They have a tendency for the eye to cause new blood vessels to grow—and in the front of the eye, these new vessels can clog the outflow of normal eye fluids. The eye pressure goes up and glaucoma develops. In the back of the eye, new blood vessels may cause bleeding.
When there is ischemic CRVO with new vessels, anti-VEGF injec- tions lead to prompt, but often temporary, control of the new ves- sels. Laser treatment tends to offer a more permanent effect. In some cases, both treatments are used.
Non-ischemic CRVO can worsen and become ischemic, so when CRVO is diagnosed, monthly checkups are initially recommended.
It’s important to note that early detection of macular edema or abnormal blood vessels is important; most patients can avoid severe vision loss if treatment is begun before substantial damage develops in the eye.
S YMPT OMS
Mild CRVO may show no symptoms. However:
- Many patients with CRVO have symptoms such as blurry or distorted vision due to swelling of the center part of the retina, known as the
- Some patients have mild symptoms that wax and wane, called transient visual
Patients with severe CRVO and secondary complications such as glaucoma (a disease characterized by increased pressure in the eye) often have pain, redness, irritation and other problems.
Bibliography
THANK YOU TO THE AUTHORS
Sophie J. Bakri, MD Audina Berrocal, MD
Thomas Ciulla, MD, MBA Geoffrey G. Emerson, MD, PhD Roger A. Goldberg, MD, MBA Dilraj Grewal, MD
Larry Halperin, MD Vi S. Hau, MD, PhD
G. Baker Hubbard, MD Talia R. Kaden, MD
M. Ali Khan, MD
Mathew J. MacCumber, MD, PhD Timothy G. Murray, MD, MBA Oded Ohana, MD, MBA Jonathan L. Prenner, MD
Carl D. Regillo, MD, FACS Naryan Sabherwal, MD Sherveen Salek, MD Andrew P. Schachat, MD Michael Seider, MD
Janet S. Sunness, MD Edward Uchiyama, MD Allen Z. Verne, MD Christina Y. Weng, MD, MBA Yoshihiro Yonekawa, MD
EDIT OR
John T. Thompson, MD
MEDICAL ILL US TRAT OR
Tim Hengst
Copyright © The Foundation American Society of Retina Specialists
Committed to improving the quality of life of all people with retinal disease.
Recent Posts
-
 Understanding Vitreoretinal Surgery: Comprehensive Eye Care at Nishant Taneja
24-Nov-2025
Understanding Vitreoretinal Surgery: Comprehensive Eye Care at Nishant Taneja
24-Nov-2025
-
 Trabeculectomy: A Key Solution for Glaucoma Management
24-Nov-2025
Trabeculectomy: A Key Solution for Glaucoma Management
24-Nov-2025
-
 Enhance Your Eye Health and Appearance with Oculoplasty Surgery at Nishant Taneja Eye Clinic in Tirana
29-Jul-2024
Enhance Your Eye Health and Appearance with Oculoplasty Surgery at Nishant Taneja Eye Clinic in Tirana
29-Jul-2024
-
 Correcting Eye Misalignment with Strabismus Surgery at Nishant Taneja Indian Eye Institute & Laser Center
29-Jul-2024
Correcting Eye Misalignment with Strabismus Surgery at Nishant Taneja Indian Eye Institute & Laser Center
29-Jul-2024
-
 Say Goodbye to Glasses! Glasses Removal at Nishant Taneja Indian Eye Institute & Laser Center
29-Jul-2024
Say Goodbye to Glasses! Glasses Removal at Nishant Taneja Indian Eye Institute & Laser Center
29-Jul-2024